Just translated nirvikalpa from a critical realist perspective with the help of Prof Sharma during our co passenger bus journey to Narketpally!
Kalpa is in the middle perceptual circle, which means individual thoughts from individual perceptions
Vikalpa is the collective cognitive options to the individual's thoughts and forms the second outer actual circle
Nirvikalpa is the outermost circle of reality where both the individual and collective merge in singularity
More shared earlier here: https://medicinedepartment.blogspot.com/2024/10/critical-realist-pedagogy-and-theatre.html?m=1
And reposted below:
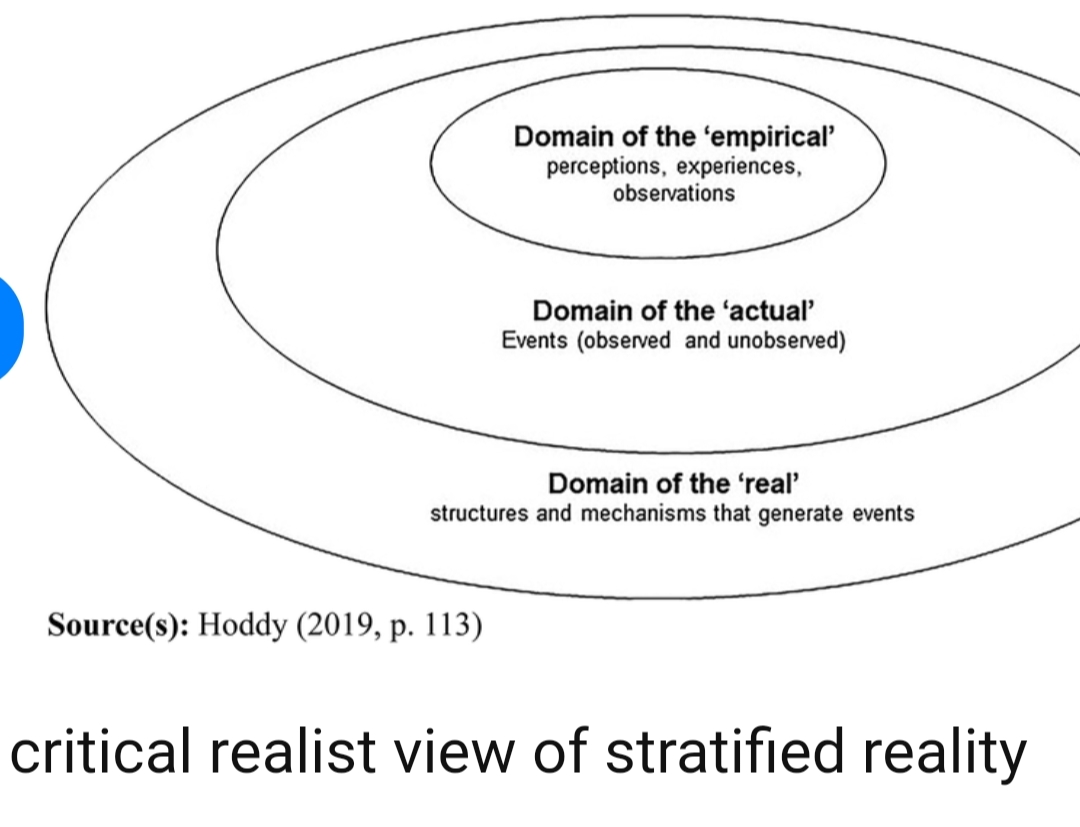
While we don't have a ©️ on the very useful figure of critical realist view of stratified reality shared by Hoddy et al : Source: https://www.
we would like to add our own diagram as a positive contribution to expand on their viewpoint from a medical cognition lens and the essence of it is all about the individual patient's and physician's cognition at the centre of the concentric circles corresponding to Hoddy's domain of the 'empirical' as in perceptions, experiences and observations of 'individual cognition' while the surrounding concentric circle forms a ring of 'actual collective cognition' that tries to tie together all knowledge elements into an 'ontology' many of which are unknown and form the connecting link to the next ring which is Hoddy's domain of the 'real' that contains all the structures and mechanisms that generate events that again feed back cyclically into the central concentric circle of individual perception of empirical events surrounded by the ring of collective cognitive interpretation of 'actual' events.

This co creation has enabled healthcare educator practitioners to not only remain focused on real patient care centred learning outcomes but develop realist ontologies for medical education and practice such as "real patient OSCEs" that retain whole patient clinical complexity rather than reduce it to smaller parts in order to optimize clinical complexity.